Great topic, **Pasindu** — axis deviation is **pure pattern recognition + logic**, and once you learn one clean algorithm, you’ll never forget it.
I’ll give you a **simple stepwise method**, then **clinical interpretation**, and finally **ICU/cardiac relevance**.
---
# ❤️ **How to Identify Cardiac Axis Deviation on ECG (Simple Algorithm)**


---
## 🧠 CORE IDEA (1 sentence)
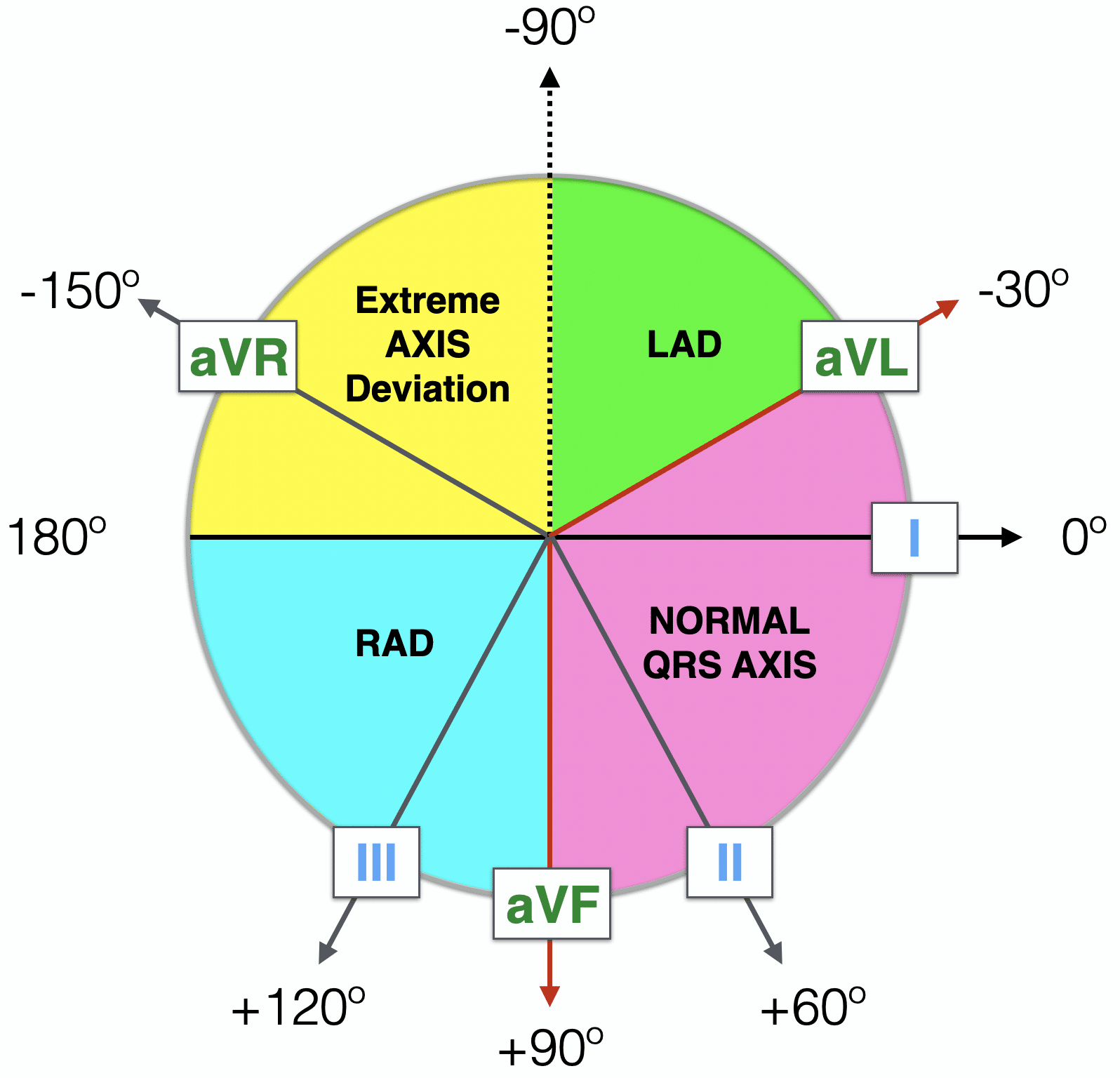
> **Axis = direction of mean ventricular depolarization in the frontal plane**
You only need **TWO leads** to identify it quickly:
👉 **Lead I** and **aVF**
---
# 🔹 STEP-BY-STEP AXIS IDENTIFICATION (FAST METHOD)
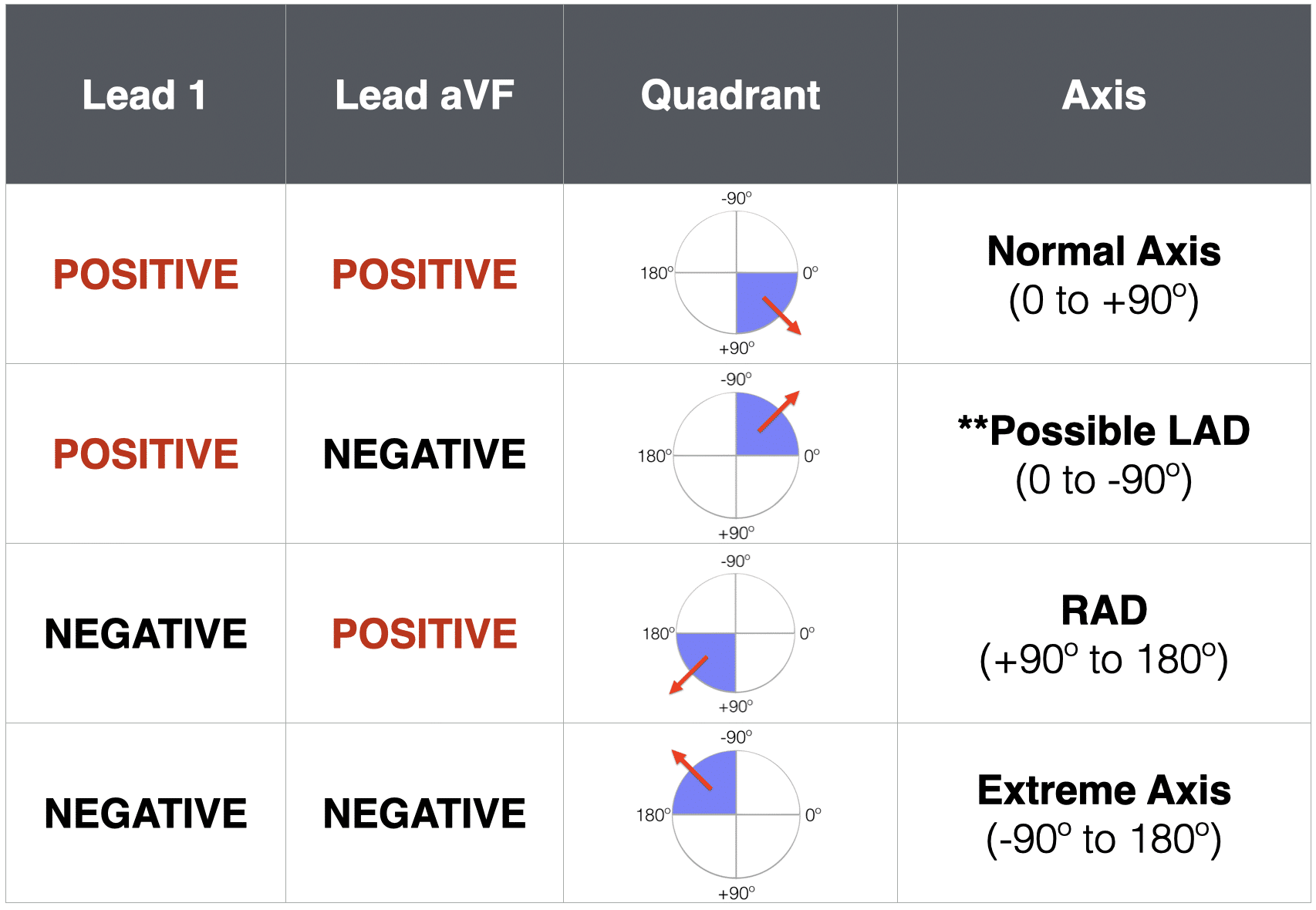
## ✅ **STEP 1: Look at QRS in LEAD I**
* **Positive (upright)** → axis points LEFT
* **Negative (downward)** → axis points RIGHT
---
## ✅ **STEP 2: Look at QRS in LEAD aVF**
* **Positive (upright)** → axis points DOWN
* **Negative (downward)** → axis points UP
---
## 🔹 STEP 3: COMBINE THE TWO → AXIS QUADRANT
| Lead I | aVF | Axis | Name |
| ------ | --- | ------- | ------------------------------ |
| + | + | Normal | **Normal Axis** |
| + | – | Left | **Left Axis Deviation (LAD)** |
| – | + | Right | **Right Axis Deviation (RAD)** |
| – | – | Extreme | **Northwest / Extreme Axis** |
That’s it.
No angles needed at bedside.
---
# 📐 OPTIONAL: ANGLE RANGES (FOR EXAMS)
| Axis | Degree |
| ------- | ------------- |
| Normal | –30° to +90° |
| LAD | –30° to –90° |
| RAD | +90° to +180° |
| Extreme | –90° to –180° |
---
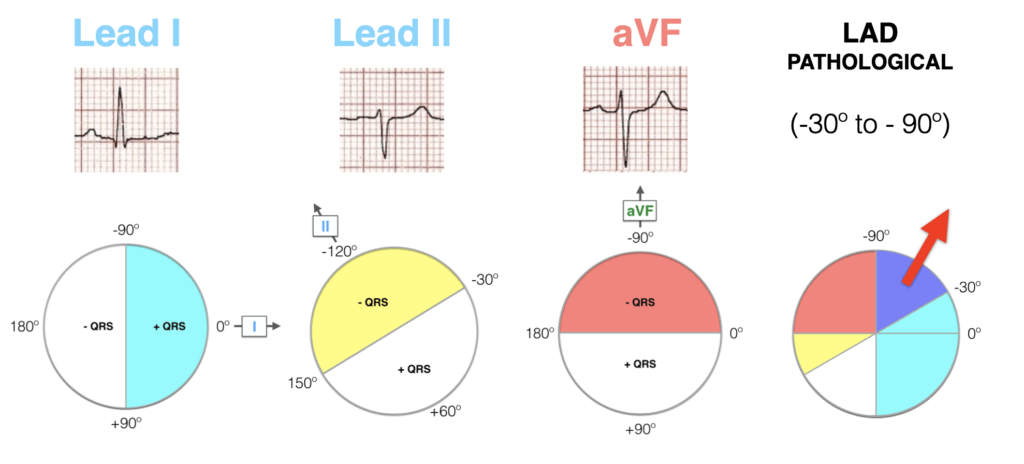
# 🔍 STEP 4 (OPTIONAL): CONFIRM BORDERLINE LAD WITH LEAD II
If:
* Lead I = positive
* aVF = negative
→ Look at **Lead II**
| Lead II | Interpretation |
| -------- | -------------- |
| Positive | Normal variant |
| Negative | **True LAD** |
---
# 🩺 CLINICAL CAUSES (VERY IMPORTANT FOR YOU)
---
## 🔵 **LEFT AXIS DEVIATION (LAD)**
### ECG pattern
* Lead I positive
* aVF negative
* Lead II often negative
### Common causes
* **Left ventricular hypertrophy**
* **Left anterior fascicular block (LAFB)** ← very common
* Inferior MI (old)
* **Aortic stenosis**
* Hypertensive heart disease
* LBBB
👉 **In cardiac patients, LAD = think LV pressure overload or conduction disease**
---
## 🔴 **RIGHT AXIS DEVIATION (RAD)**
### ECG pattern
* Lead I negative
* aVF positive
### Common causes
* **Right ventricular hypertrophy**
* Pulmonary hypertension
* Pulmonary embolism
* COPD
* Left posterior fascicular block
* Normal in children & thin adults
👉 **In ICU: acute RAD = think PE or RV strain**
---
## ⚫ **EXTREME AXIS (VERY ABNORMAL)**
### ECG pattern
* Lead I negative
* aVF negative
### Causes
* Ventricular rhythms (VT)
* Severe hyperkalaemia
* Emphysema
* Ventricular pacing
* Congenital heart disease
👉 **Extreme axis = usually ventricular origin or severe pathology**
---
# 🧠 MEMORY TRICK (VERY EASY)
### **“Two Thumbs Rule” 👍👍**
* **Lead I = left thumb**
* **aVF = down thumb**
| Thumbs Up | Axis |
| --------- | ------- |
| 👍 👍 | Normal |
| 👍 👎 | Left |
| 👎 👍 | Right |
| 👎 👎 | Extreme |
---
# 🔑 ICU & CARDIAC SURGERY PEARLS
* **New axis deviation = pathology until proven otherwise**
* **Post-op LAD** → think conduction injury (LAFB)
* **Sudden RAD** → think PE, RV failure, tamponade
* **Wide QRS + extreme axis** → VT until proven otherwise
* Axis deviation helps **localize disease**, not diagnose alone
---
# 🧾 QUICK ONE-LOOK SUMMARY
| Axis | Lead I | aVF | Think of |
| ------- | ------ | --- | ----------------- |
| Normal | + | + | Normal / athletic |
| LAD | + | – | AS, LVH, LAFB |
| RAD | – | + | PE, RV strain |
| Extreme | – | – | VT, hyperK |
---
## 🎯 TAKE-HOME
> **Axis = Lead I + aVF**
> If you can read those two leads, you can identify axis in **5 seconds**.
---
If you want next, I can give you:
* 🔹 **Axis deviation ECG flashcards**
* 🔹 **Axis deviation + bundle branch block combined interpretation**
* 🔹 **Axis deviation in ICU emergencies (PE, VT, hyperkalemia)**
Just tell me what you want next 👍
No comments:
Post a Comment