Here we go, **Pasindu** — aortic stenosis (AS) has **no single diagnostic ECG pattern**, but it produces a **cluster of changes** due to *pressure overload → concentric LV hypertrophy → strain → conduction abnormalities*.
So your job is to recognize the **ECG “fingerprints”** of a pressure-loaded left ventricle.
Below is a **clean, systematic, clinician-friendly guide**.
---
# 🔵 **How to Identify Aortic Stenosis on ECG**

---
# ✅ **Core Concept:
Aortic stenosis does NOT have a specific ECG pattern.
But it causes ECG changes secondary to *LV pressure overload*.**
So you identify AS on ECG by spotting patterns of:
### **1. Left Ventricular Hypertrophy (LVH)**
### **2. LV strain pattern (ischaemia due to hypertrophy)**
### **3. Conduction delays (especially LBBB)**
### **4. Left atrial enlargement**
When you see these *together*, think “AS until proven otherwise."
---
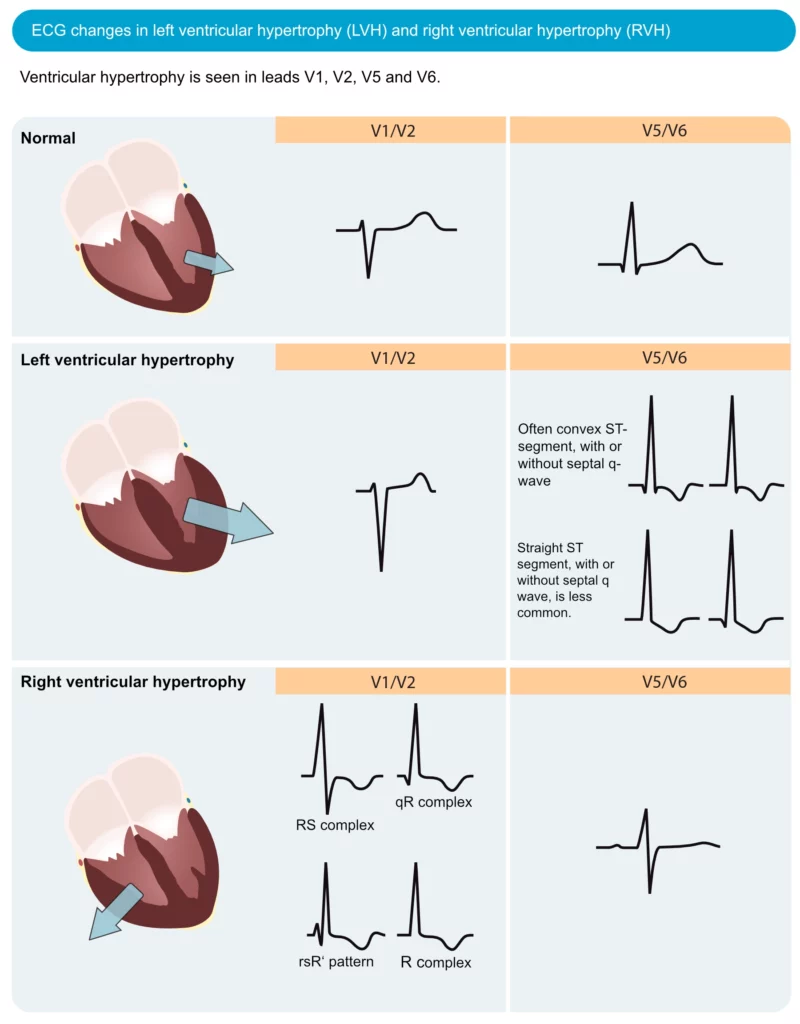
# 🔹 **1. LVH Voltage Criteria (Most Common)**
The LV becomes thick due to chronic pressure load → **tall left-sided voltages**.
### **Sokolow-Lyon Criteria**
* **S in V1 + R in V5 or V6 ≥ 35 mm**
### **Cornell Criteria**
* **R in aVL + S in V3 > 28 mm (men)**
* **> 20 mm (women)**
### **Other ECG clues**
* Tall R waves in **I, aVL, V5–V6**
* Deep S waves in **V1–V3**
* Left axis deviation (sometimes)
**If you see “big voltages everywhere” → think LVH → suspect AS.**
---
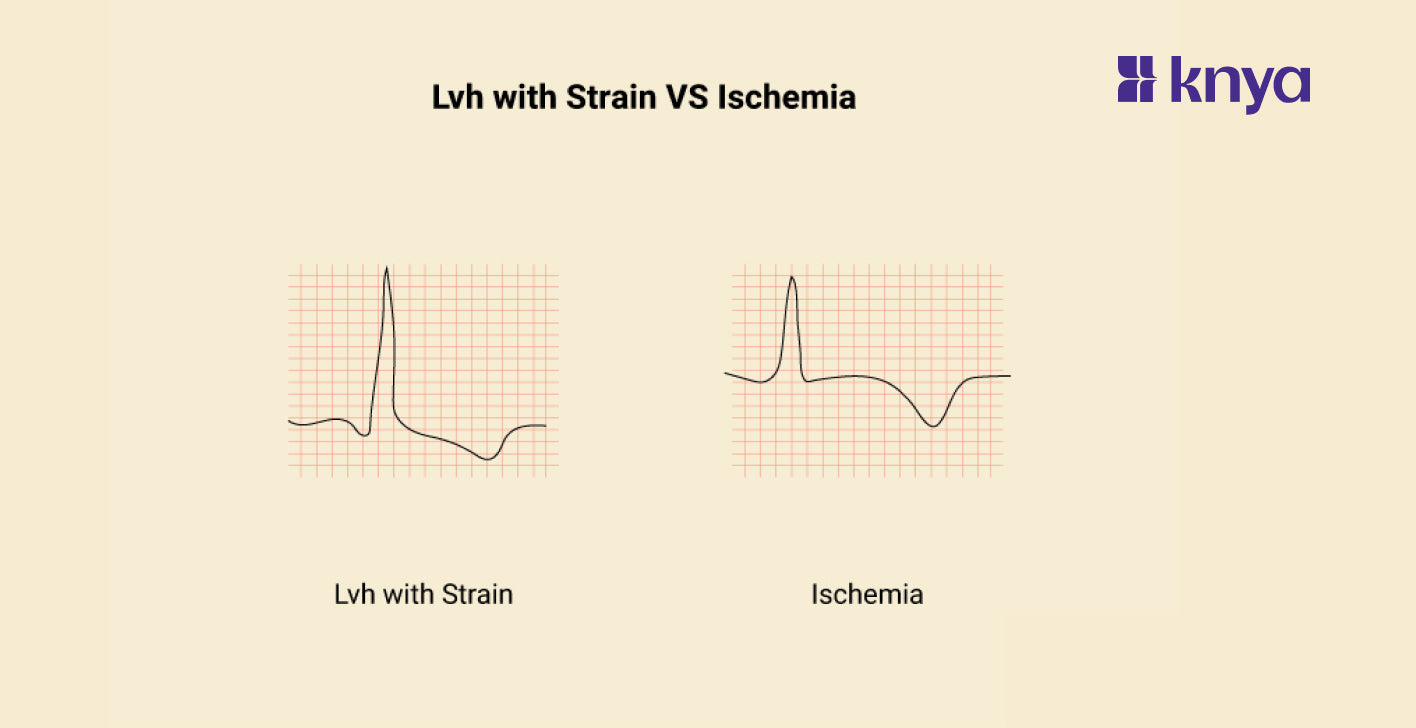
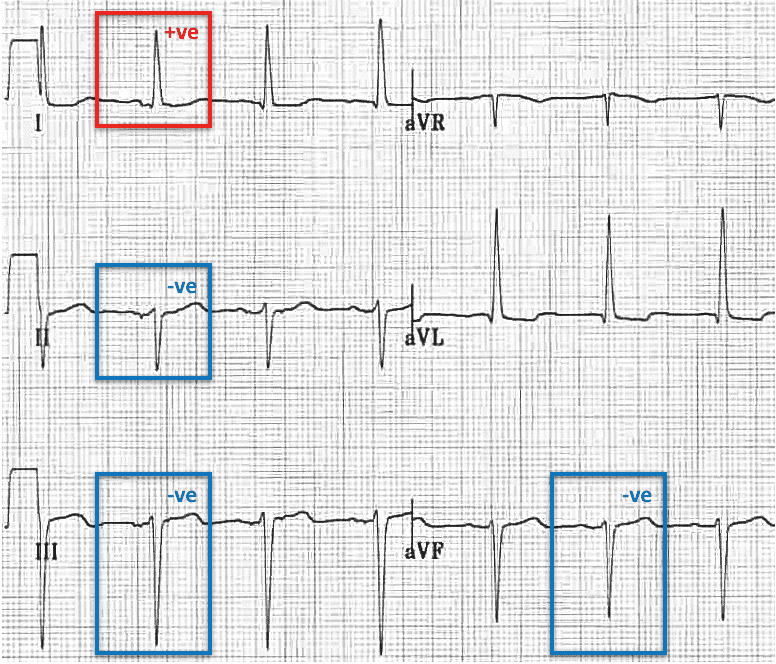
# 🔹 **2. LV Strain Pattern (Very Suggestive of Severe AS)**
Due to subendocardial ischaemia from pressure overload.
### **Typical findings:**
* **ST depression and T-wave inversion** in
* **Lateral leads:** I, aVL, V5, V6
* Sometimes inferior leads
* Downsloping ST segment
* Asymmetric T-wave inversion
This is called the **LV strain pattern**, and in an older patient it is highly predictive of **severe AS**.
👉 **LVH + strain pattern = strong hint of severe aortic stenosis.**
---
# 🔹 **3. Left Atrial Enlargement (LAE)**
Due to chronically elevated LV end-diastolic pressures.
### **ECG clues:**
* Broad, notched P wave in lead II (“P mitrale”)
* Biphasic P wave in V1 with large negative terminal portion
LAE + LVH strongly supports AS physiology.
---
# 🔹 **4. Conduction Abnormalities Seen in AS**
**LBBB** or **1st-degree AV block** may appear due to septal thickening or calcified valve extending into conduction tissue.
Common patterns:
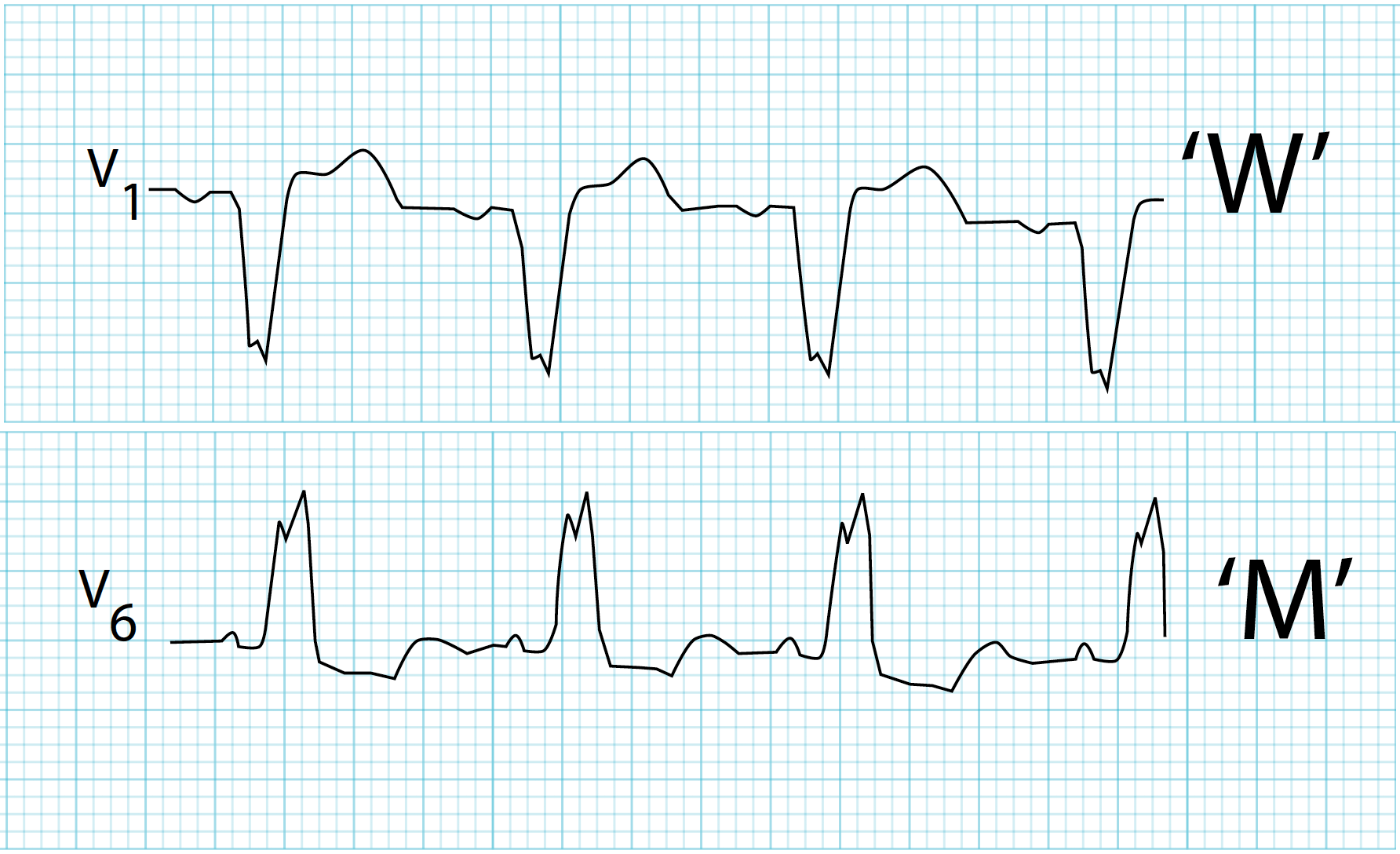
* **Left Bundle Branch Block**
* **Left anterior fascicular block (LAFB)**
* **1° AV block (PR > 200 ms)**
**Severe calcific AS** → can progress to higher-degree AV block (rare).
---
# 🔹 **5. Rhythm Abnormalities Associated with AS**
* **Atrial fibrillation** is dangerous in AS because these patients rely heavily on atrial kick; AF may be the first presenting ECG clue.
* Frequent **ventricular ectopics** due to hypertrophied myocardium.
---
# 🔹 **6. What Severe AS ECG Usually Looks Like (Clinically)**
You’ll typically see some combination of:
### 🔥 **“Triple sign” of severe aortic stenosis on ECG:**
1. **LVH by voltage**
2. **LV strain pattern** in lateral leads
3. ± **Left atrial enlargement**
If an older patient has this → *think calcific severe AS*.
---
# 🔹 **7. What ECG Does NOT Show (Important)**
* **ECG CANNOT diagnose AS severity**
* **ECG CANNOT exclude AS**
* 20–25% of severe AS patients have completely normal ECGs
So ECG is **suggestive**, not diagnostic.
**Echo** is always required.
---
# 🔹 **8. Quick Memorization Mnemonic — “AS = LV PRESSURE”**
**P**ressure overload → LVH
**R**epolarization abnormality → strain
**E**nlarged left atrium
**S**low conduction (LBBB, 1° block)
**S**tiff ventricle → AF risk
**U**psloping voltages
**R**ight leads deep S waves
**E**xtension of calcification to conduction system
---
# 🔹 **9. Summary Table**
| ECG Finding | Meaning | Why in AS |
| -------------- | --------------------------- | --------------------------------- |
| LVH voltage | Tall R in I, aVL, V5–V6 | LV pressure overload |
| LV strain | ST↓ & T inversion (lateral) | Subendocardial ischemia |
| LA enlargement | Broad P wave | High filling pressure |
| LBBB | Conduction delay | Septal thickening / calcification |
| AF | Irregular rhythm | LA pressure + fibrosis |
---
# 🔵 **Takeaway for Cardiac Practice**
> If ECG shows **LVH + strain**, especially in an elderly patient with systolic ejection murmur → **assume severe AS until echo proves otherwise**.
---
If you want, I can now create:
### 🔸 A side-by-side **ECG comparison sheet** (normal vs AS vs LV strain)
### 🔸 A **one-page pocket reference** for all valvular ECG patterns
### 🔸 AS ECG identification **flashcards for memorizing**
Just tell me which format you prefer.
No comments:
Post a Comment